
September 2020 - Presented by Dr. Anupam Mitra (Mentored by Dr. John Bishop)
Clinical history
A female in her mid-50s presented with a gradually increasing painful vulvar mass for last 8 months. She denies fever or chills, vaginal discharge or bleeding, abdominal pain, nausea, vomiting, weight loss and change in bowel/bladder function. Patient had a long history of intermittent cysts in the vulva and received several treatments. She told that her previous cysts looked different compared to this vulvar mass. She also had a history of long-standing endometriosis for which supracervical hysterectomy was done almost two decades ago. Recent PAP was negative for intraepithelial lesion or malignancy, and HPV was negative too. She underwent radical vulvectomy for this vulvar mass.
Imaging findings
MRI of the pelvis showed a multilobulated heterogeneously enhancing soft tissue mass within the mons pubis with prominent inguinal lymph nodes and an indeterminate left common iliac lymph node (Figure 1). The mass and lymph nodes were FDG-avid on PET scan.
Macroscopic findings
An ovoid multilobulated grey-white fleshy mass (8.0 x 6.5 x 4.7 cm) with a smooth and thin encapsulation. Majority of the mass is in the subcutaneous tissue with approximately 20% protruding through the overlying skin surface as a red congested umbilicated nodule (2.1 cm in diameter).
Microscopic findings
H&E of the lesion shows predominantly papillary architecture with focal areas of necrosis and interconnecting vascular network (Figure 2). The tumor cells are mostly cuboidal and hobnail type with nuclei protruding into the lumen and arranged in sheets and papillae (Figure 3). Tumor cells have abundant granular eosinophilic to clear vacuolated cytoplasm. Hyaline globules are seen. Nuclei are pleomorphic, irregular, and have frequent prominent nucleoli (Figure 4).
Ancillary testing
A panel of immunohistochemical (IHC) stains was performed on the resection specimen to further characterize the neoplasm (Figure 5).
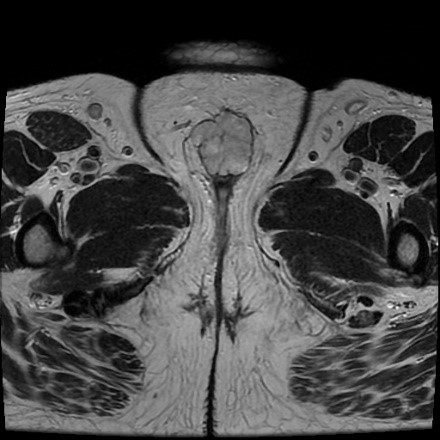
Figure 1: MRI of the pelvis.
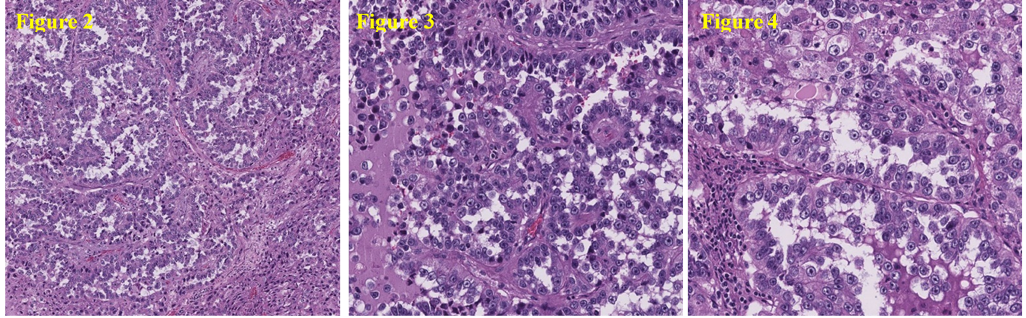
H&E staining of the tissue: Low magnification view of the tumor’s papillary growth pattern (Figure 2). High magnification view of mostly cuboidal and hobnail tumor cells (Figure 3). High magnification view of pleomorphic nuclei with prominent nucleoli and hyaline globule (Figure 4).
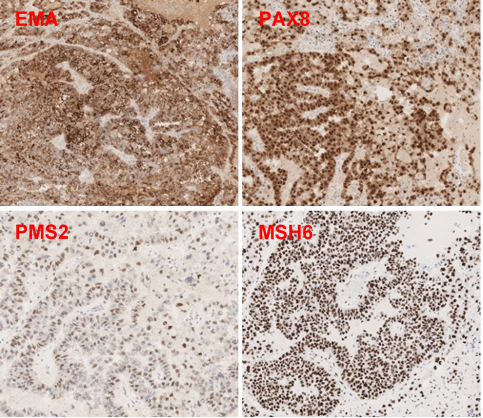
Figure 5: IHC staining of the tissue. Tumor cells are POSITIVE for EMA and PAX8. Tumor cells have INTACT (normal) PMS2 and MSH6.
B.) Endometriosis
 Meet our Residency Program Director
Meet our Residency Program Director
 LeShelle May
LeShelle May Chancellor Gary May
Chancellor Gary May