
Residency Program - Case of the Month
November 2016 - Presented by Dr. Ananya Datta Mitra
Clinical History
The patient is a 70 year old Caucasian male, who is transferred from an outside institution with complains of increasing black stools, fatigue, nausea and vomiting and vague upper abdominal pain. He states that his symptoms have been present for the past two months and he has been having fatigue, light headedness and weight loss. He denied H/O fever, jaundice, change in bowel movements, lymphadenopathy, night sweats, shortness of breath and chest pain.
Past medical history is significant for alcohol abuse (heavy drinking history, six pack per week of beer), smoking (50 PPD smoking history) and drugs (marijuana). There is no family history of gastrointestinal (GI) malignancy and there is no history of recent travel.
Physical exam findings include a nondistended abdomen with mild tenderness, no fluid thrill, and no hepatosplenomegaly. There is no jaundice, pedal edema or any skin changes.
Imaging
He underwent a CT abdomen which showed diffuse gastric wall thickening and heterogeneity involving the distal gastric body and antrum with mild adjacent haziness, compatible with history of stomach mass. Additionally there is a hypoattenuating linear track-like cleft along the inferior gastric wall which has the appearance of a possible healing ulceration.
Click to enlarge image
| Figure 1 |
 |
Upper GI endoscropy (EGD)
EGD reports that there is a massive ulcer in the antrum near the pylorus that encircles more than half of the way around the lumen and appeared malignant, several biopsies are taken. However, before the biopsy results the patient is transferred to UC Davis Medical Center.
Gross findings
The patient underwent subtotal gastrectomy. The stomach is opened longitudinally to reveal a large circumferential tumor measuring 14.5 x 10.5 x 2.1 cm. The overlying mucosa is flattened, with loss of the normal rugal folds. On cut surface the tumor invades into the muscularis propria.
Click to enlarge image
| Figure 2 |
 |
Microscopic findings
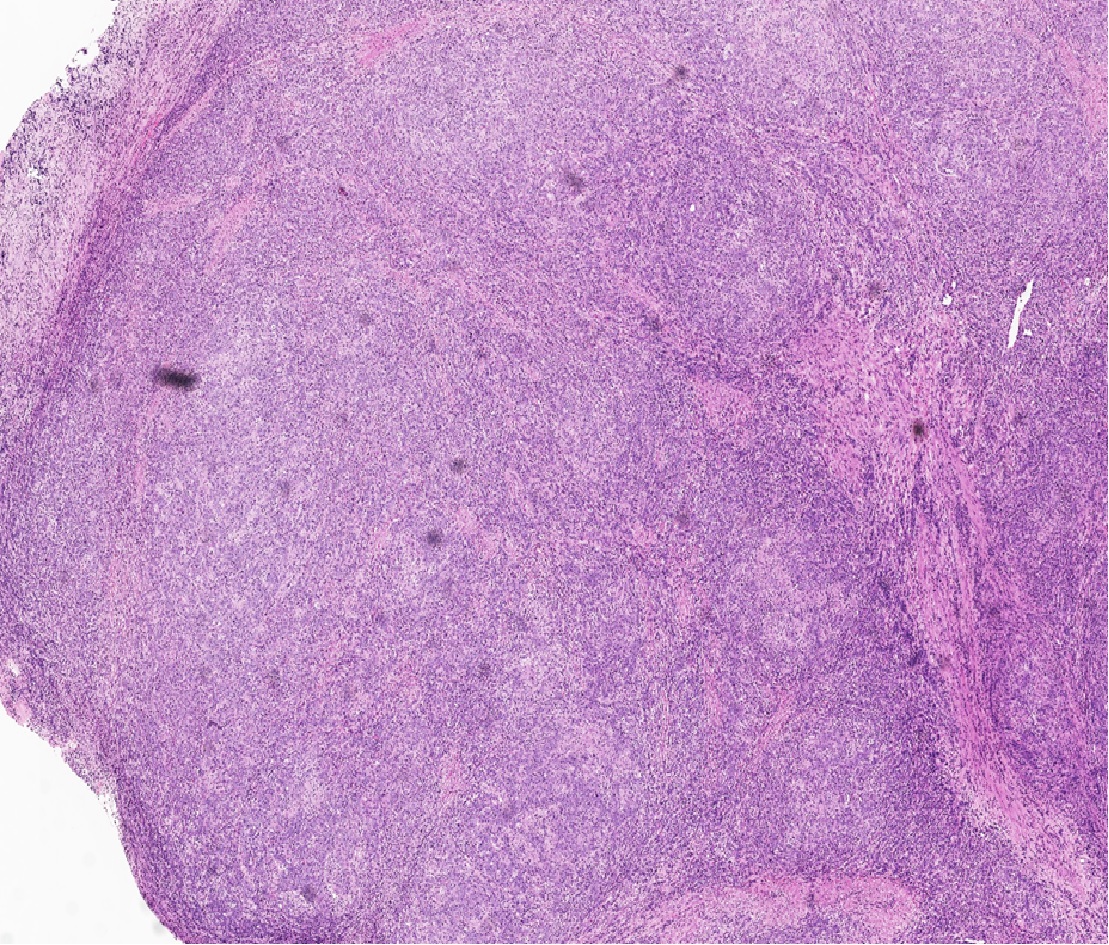
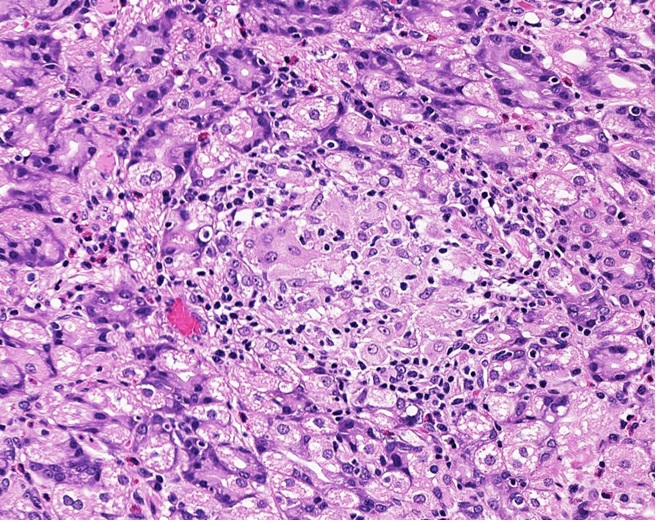
Microscopically, the tumor is composed of sheets and nests of round to polygonal cells with poorly defined cell borders within a dense lymphocytic background (Figure 3A-B).
Click to enlarge image
| Figure 3A | Figure 3B | |
 |
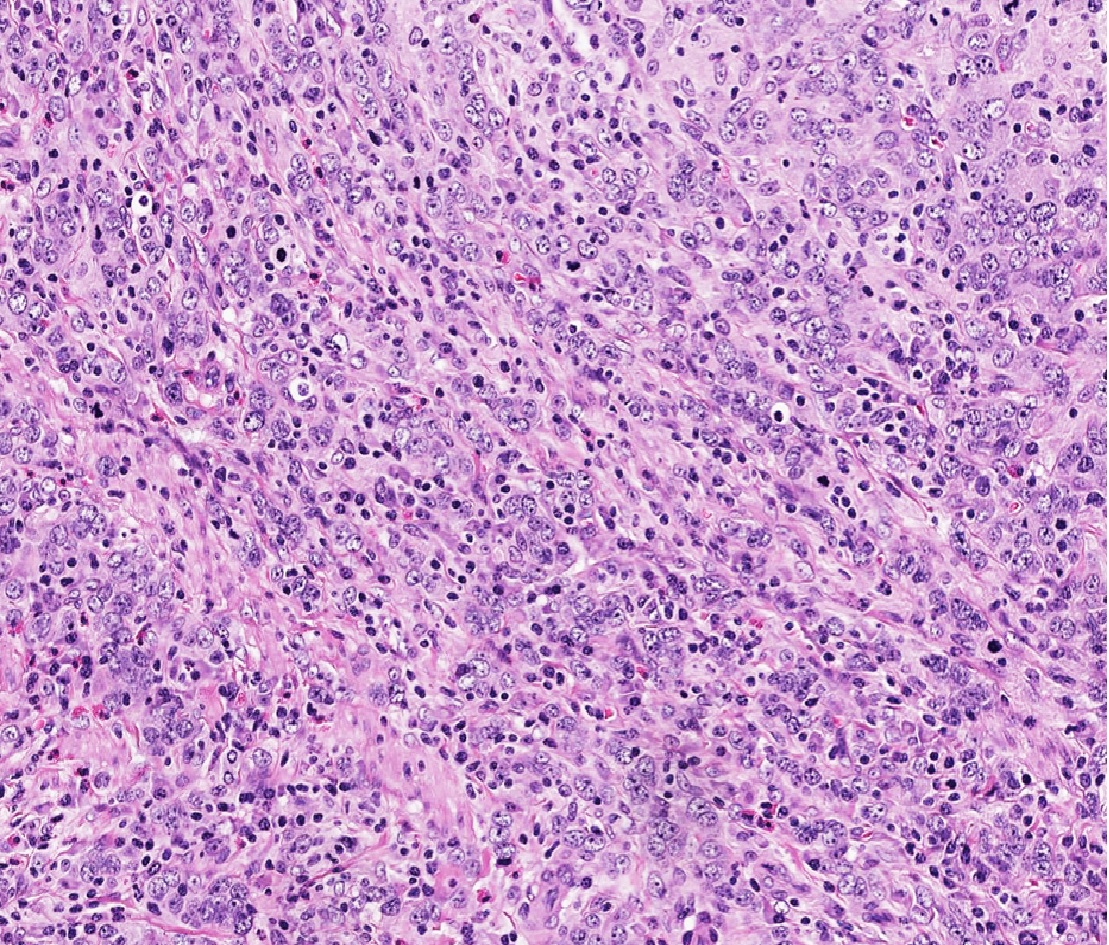 |
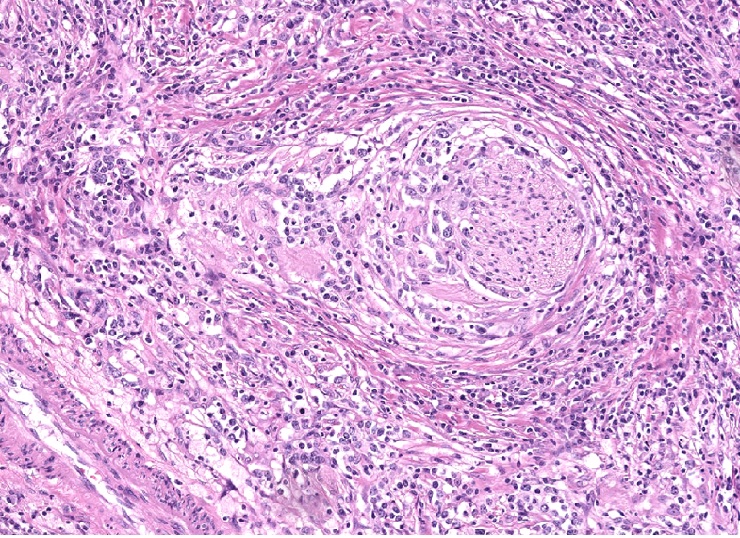
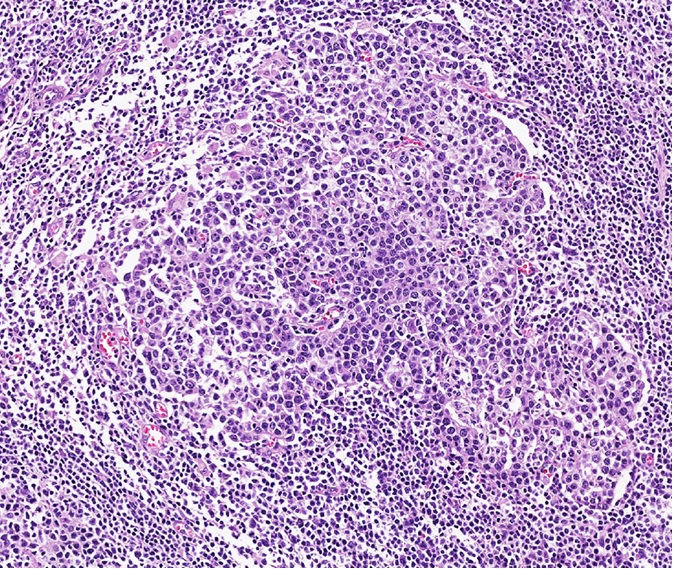
Cytologically, the tumor cells are large and pleomorphic with abundant eosinophilic cytoplasm, large vesicular nuclei and prominent nucleoli. Perineural invasion (Figure 3C) and lymph node invasion is observed (Figure 3D). There are scattered epitheloid granulomas (Figure 3E), AFB and GMS negative.
Click to enlarge image
| Figure 3C | Figure 3D | Figure 3E | ||
 |
 |
 |
Immunohistochemical staining
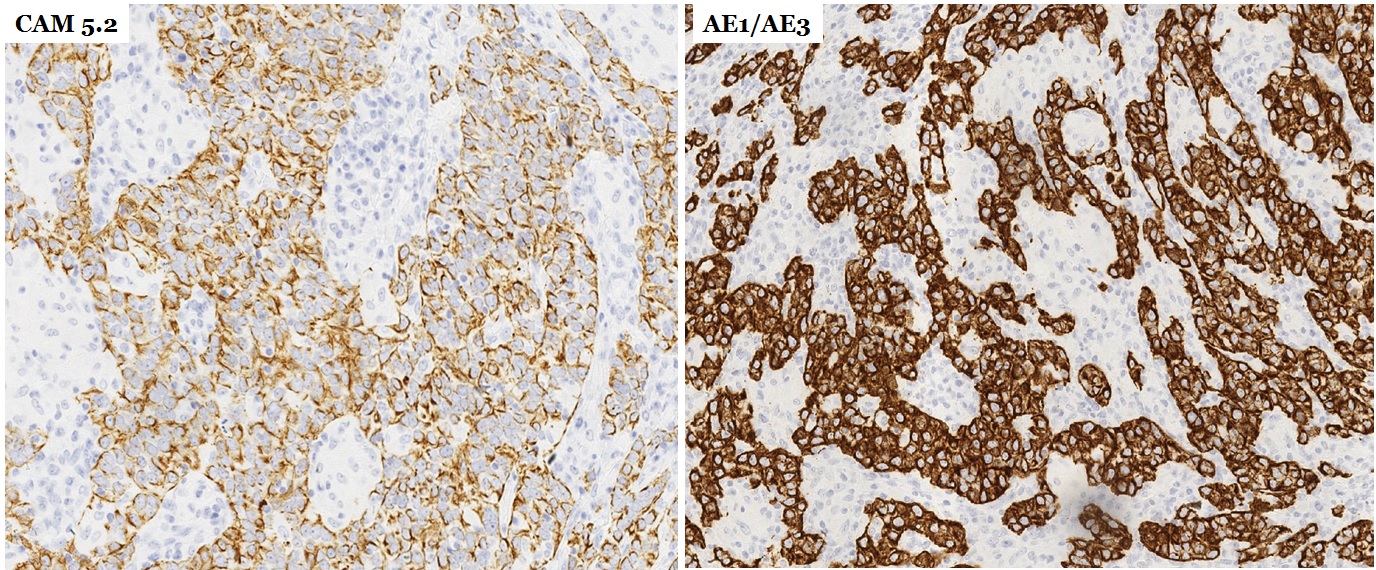
Immunohistochemical staining for pan-cytokeratin (CAM5.2 and AE1/AE3) is positive (Figure 4A).
Click to enlarge image.
| Figure 4A |
 |
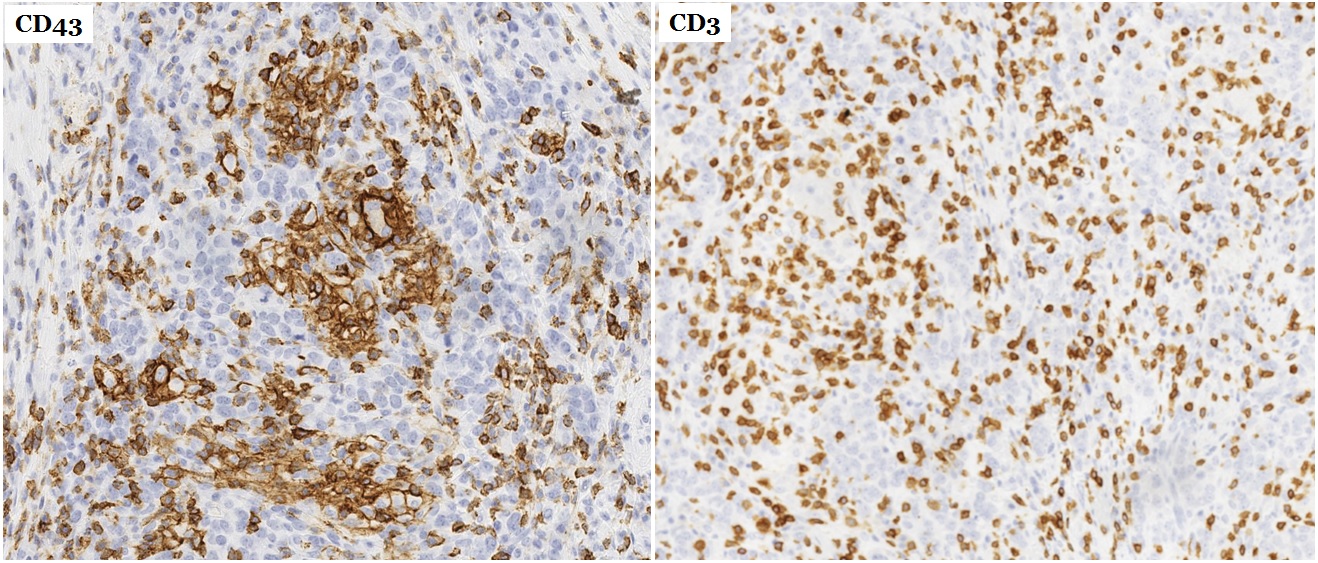
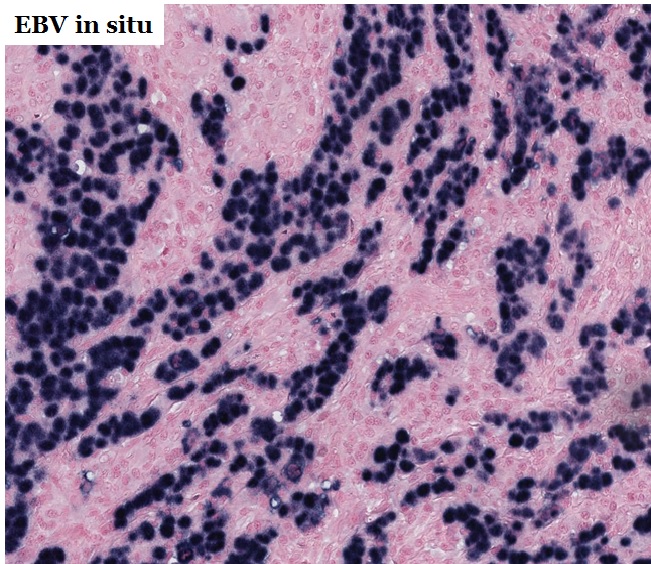
There are abundant intratumoral T cells highlighted by CD3 and CD43 (Figure 4B). The tumor is negative for CD20, S100. The in situ hybridization for EBV-encoded small RNAs (EBER-1 and 2) showed an intensive nuclear hybridization signal corresponding to the carcinoma cells. No EBV hybridization signal evident in the adjacent non-neoplastic gastric mucosa, in the lymphocytes around the tumor cell or in the dissected lymph nodes. (Figure 4C)
Click to enlarge image.
| Figure 4B | Figure 4C | |
 |
 |
What is the diagnosis?
Choose one answer and submit.
E. Gastric lymphoepithelioma-like carcinoma or medullary carcinoma
> Learn more about this diagnosis.
 Meet our Residency Program Director
Meet our Residency Program Director
 LeShelle May
LeShelle May Chancellor Gary May
Chancellor Gary May